History:
Female patient 12 years old complaining of nasal obstruction, hyposmia and nasal discharge. No history of previous operation or medication.
Examination:
Local examination of the face showing adenoid faces, slit shaped nostril opening, prominant central incisor, dry cracked lips, obliterated nasolabial fold and high arched palate with teeth crowding. Anterior nasal endoscoy by nasal speculum showed bilateral nasal masses, pale greyish in color, attached to lateral nasal wall. Anterior nasal endoscopy showed the nasal masses protruding from middle meatus and superior meatus and polypoidal middle turbinate and enlarged adenoid.
Investigation:
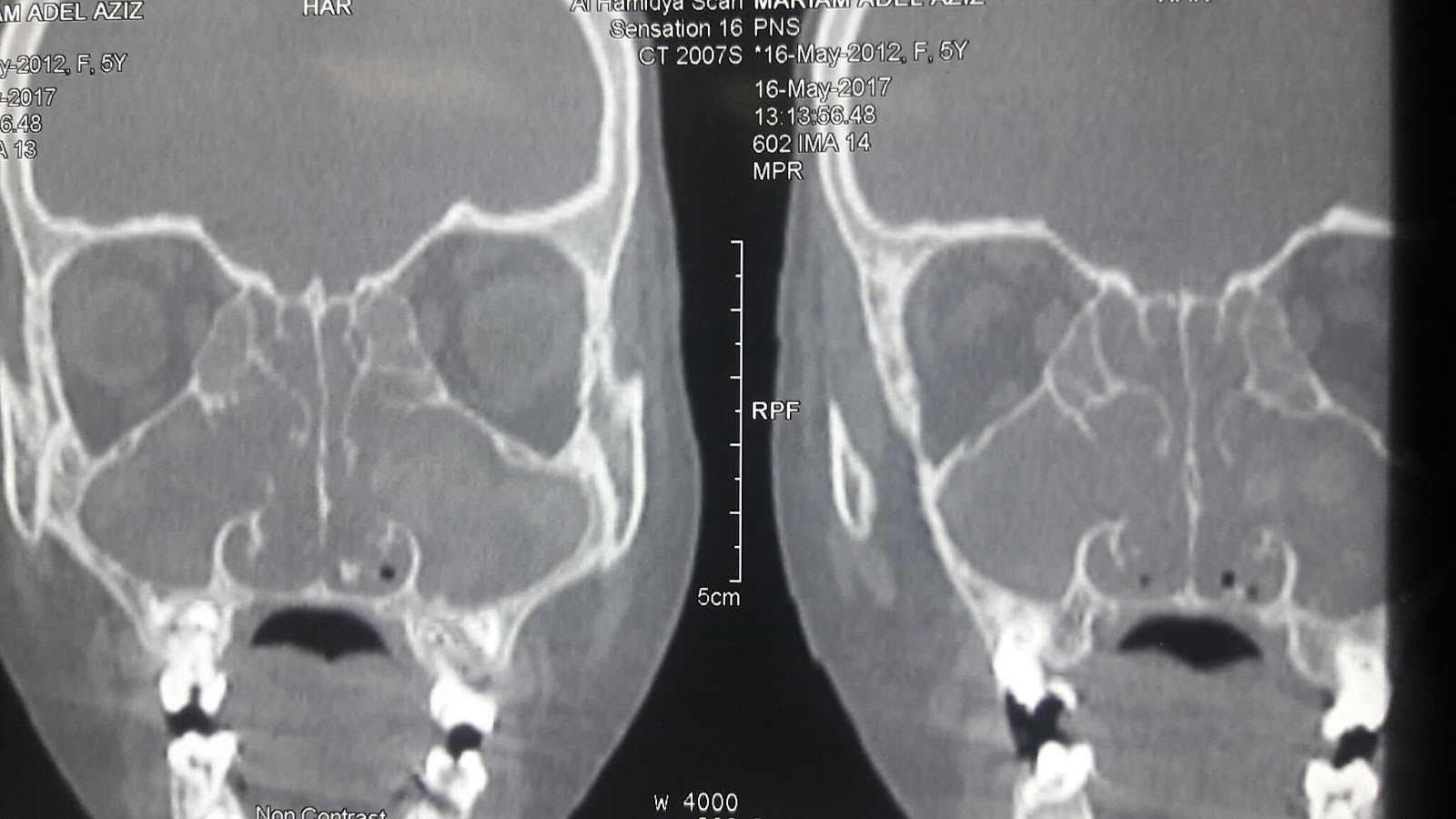
CT scan nasal and paranasal sinuses axial, coronal and saggital cutts showed bilateral soft tissue density on both side of the nasal cavity and occupying anterior, posterior ethmoid and maxillary sinuses.
This density is heterogenous and contains hyperdense foci giving motteled appearance most probably due to fungus infection.
This hyperdense foci due to minerals produced by the fungus like magnesium and iron. There is also bone remodling of the sinuses. Other laboratory investigation done like taking biopy from the nasal mass for fungal stain and culture which reveal septate hyphea with 45 degree angle septation. The fungus was aspergillus. Ige specific to the fungus detected in blood, which confirm diagnosis of allergic fungal rhinosinusitis. Other laboratoy investigation to prepare the patient to the nasal sinus surgery. Allergic fungal rhinosinusitis may be a part of allergic pulmonary aspergellosis. So we have to look at the chest to exclude this entity.
Differential diagnosis:
This age of patient with nasal polyp make us thinking about other causes of nasal polyps in children like cystic fibrosis, immotile cilia syndrome, ciliary dyskinesia, samter triade. Cystic fibrosis is diagnosed by sweat chloride test, immotile cilia syndrome is diagnosed by brush biopsy and cytological examination and saccharine test. Samter triade is suspected if there is history of aspirin sensitivity.
Management:
Patient prepared for endoscopic sinus surgery. Hypotensive technique done and local vasoconstrictor drops applied. ESS steps are uncinectomy, middle meatal antrostomy, anterior and posterior ethmoidectomy. Nasal packs putted after operation for 2 days.


{kind=link}
تعليقات
إرسال تعليق
أكتب تعليقك او استفساراتك وسيتم الرد من قبل استشارى متخصص في جراحات وامراض الانف والاذن والحنجرة وتجميل الانف والوجه